

Background:
Post-partum hemorrhage (PPH) is a major cause of maternal mortality. The risk of death from PPH is approximately 1 in 1000 deliveries(Carroli et al., 2008). Tranexamic acid (TXA) is a recommended treatment for women with severe PPH as it significantly reduces blood loss, need for surgical intervention and maternal mortality from hemorrhage (Abdul-Kadir et al., 2014; Ducloy-Bouthors et al., 2011; Li et al., 2017). Despite evidence supporting the use of TXA in this setting, there remain concerns and reluctance with its use stemming from the known increased risk of venous thromboembolism (VTE) in women post-partum (Tepper et al., 2014; James, 2009). Much of the data on TXA use has come from studies conducted on women without a bleeding disorder. Women with inherited bleeding disorders are at a substantially greater risk of PPH with maternal mortality from PPH estimated to be 10 times higher than average(Abdul-Kadir et al., 2014; James & Jamison, 2007). The safety and efficacy of peri-partum use of TXA in this population warrants study given their increased baseline risk of PPH and lower risk of thromboembolism (James & Jamison, 2007; Martin & Key, 2016).
Methods:
A retrospective cohort study was conducted on all women with inherited bleeding disorders known to our Multidisciplinary Clinic for Women with Inherited Bleeding Disorders (MCWBD) who received TXA peri-partum between July 2014 and December 2019. The primary objective was to evaluate the frequency of VTE amongst patients with inherited bleeding disorders who received peri-partum TXA. The secondary objective was to evaluate the frequency of primary and secondary PPH among those who did and did not receive TXA. Research ethics board approval was obtained. Descriptive statistical analyses were used.
Results:
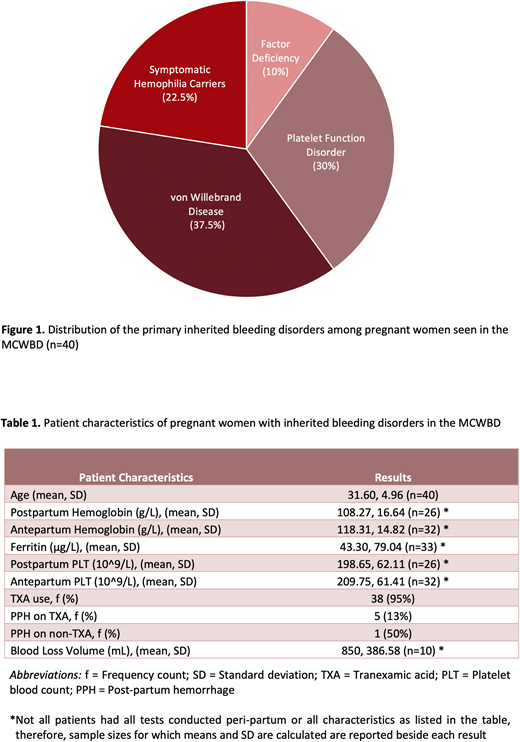
There were no VTE events in all MCWBD patients who received TXA peri-partum. A total of 40 patients with inherited bleeding disorders were managed from the beginning of pregnancy to labour and delivery under the care of the MCWBD between July 2014 and December 2019. The distribution of primary bleeding disorder diagnoses is 37.5% (15/40) for von Willebrand disease, 30% (12/40) had platelet function disorders, 22.5% (9/40) were symptomatic hemophilia carriers and 10% (4/40) had a rare factor deficiency (see Figure 1). Of these patients, 25% (10/40) had a personal previous history of PPH and 13% (5/40) had a family history of PPH. Among the 40 women, 75% (30/40) gave birth vaginally. TXA was provided to 95% (38/40) of patients at the onset of the second stage of labour, during the postpartum period (minimum of 10 days of oral TXA treatment), or both. Primary PPH occurred in 13% (5/38) of women who received prophylactic TXA and in 1 out 2 (50%) women without prophylactic TXA (see Table 1). There were no reports of secondary PPH.
Conclusions:
TXA appears to be a safe preventative treatment for PPH in patients with inherited bleeding disorders based on our retrospective study, with no additional risks of thromboembolism observed. Prospective evaluation of peripartum TXA use in this patient population is warranted to further assess its efficacy.
Martin:Borden Ladner Gervais LLP: Consultancy. Sholzberg:NovoNordisk: Honoraria, Other: Scientific Advisory Board; Novartis: Honoraria, Other: Scientific Advisory Board; Takeda: Honoraria, Other: Scientific Advisory Board, Research Funding; Amgen: Honoraria, Other: Scientific Advisory Board, Research Funding; Octapharma: Honoraria, Other: Scientific Advisory Board, Research Funding.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal